
Terms & Definitions relating to Venous Disease
Phlebology
Phlebology is the term for modern vein medicine, mostly pertaining to vein disease of the lower extremities. Even our specialty societies are now shying away from the term Phlebology due to confusion with “Phlebotomists”—phlebotomists being persons lab techs trained to draw blood. The recent explosion in interest in vein medicine by physicians and patients has been in large part due to advances in ultrasound diagnosis and laser therapy–which have dramatically simplified and improved the results of treatment of varicose vein disease–allowing much more precise treatment in a minimally invasive manner, with much lower risk, and much higher patient satisfaction. It is a relatively new field, receiving status as an independent specialty by the American Medical Association in 2005. Consequently, phlebology training is only now being incorporated in to the curriculum of some existing residency programs and medical schools. Some mini-fellowships are now offered, but most existing vein specialists learned through preceptorships with existing, more experienced physicians. Board certification was not offered until the exam became available in 2008 by the American Board of Phlebology (recently renamed: American Board of Venous and Lymphatic Medicine). Several vein societies, both in the U.S. and internationally, conduct regular meetings concentrating on disseminating information on advances in the field to vein specialists.
For more information, visit The American Board of Venous & Lymphatic Medicine or the American Vein and Lymphatic Society web sites.
 Anatomy of Leg Veins
Anatomy of Leg Veins
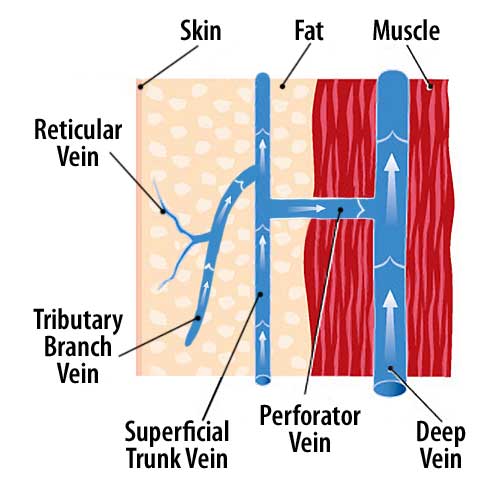
The vein drainage system of the leg is comprised of three levels that all communicate: 2 superficial levels–a system of Reticular Veins right below the skin surface, and the main superficial system that drains in to the deep vein system. The main superficial system is comprised of both Tributary Veins (also termed Branch Veins) and Trunk Veins. The two main trunk veins are the Great Saphenous and Small Saphenous Veins. Some people have other extra trunk veins that are revealed on ultrasound. The deep vein system is located in the muscles of the leg. It too has tributary veins and a large trunk vein that runs from the foot up to the groin. There is one more set of important veins of the legs termed the Perforator Veins (sometimes referred to as Connector Veins). The leg has approximately 100 of these perforator veins to connect the superficial tributary veins and trunk veins to the deep veins in the muscle.
If vein flow in the leg is proper, all blood from the superficial veins (skin level down the surface of the muscle) drains from reticular veins in to the tributary veins, then in to the trunk veins, then in to the deep veins. The great saphenous trunk vein drains in to the deep vein in the groin, and the small saphenous vein drains in to the deep veins at the back of the knee in most people. The perforator veins serve as a back-up and secondary way that drains some blood from the superficial veins in to the deep veins.

In the normal leg, the ratio of venous blood volume in the leg is 90% within the deep system and only 10% in the superficial system at any given point in time.
Since we as humans spend 2/3 of our lives upright (either sitting, standing, or walking), the vein system of the legs must have a way to get venous blood back to the heart when gravity is at play. Since we do not have a heart in the legs to pump blood against gravity, the venous blood exits the legs against gravity depending on two things: 1) the calf muscle pump, and 2) a series of hundreds of one way valves that work in concert to allow blood to move up through the legs in all levels of the vein system.
Varicose Veins
The term for the unsightly ropey and tortuous bulgy veins that you see and feel on the surface of the leg. These are actually just the visible sign of the real underlying problem of the venous circulation of the leg: Chronic Venous Insufficiency. The varicose veins are actually tributary veins (also termed branch veins) of the main draining trunk veins (usually either the Great Saphenous Vein or Small Saphenous Vein). The tributary veins become varicosed due to valve failure with subsequent backflow (also termed reflux) of too much volume of blood that ruins the integrity of the vein walls, causing these veins to bulge out, especially while the affected person is in a gravity dependent position.
Chronic Venous Insufficiency (CVI)
CVI is the real reason that most people develop chronic pain and/or swelling of the legs with or without visible varicose veins. In the vast majority of people, it is an inherited trait. Estimates are 25% – 40% of the population carries the genes for this problem, and it can skip generations. Other than heredity, a former deep vein clot and major trauma to the leg can cause CVI. Further, CVI can either be a problem in the deep veins, the superficial veins, or both. In the vast majority of people with chronic swelling, pain, and/or varicose veins of the leg, the problem is solely superficial CVI. CVI boils down to a problem in most patients to inherited faulty valves. Unlike people with normal valves, the faulty valves fail over time, such that they no longer are able to work against gravity properly. When exposed to gravity, these valves cannot hold the vein blood and buckle, allowing blood in the larger volume deep veins to backflow down one of more of the main trunk veins and usually secondarily in to one or more of the tributary veins. In contrast, even if the valves are faulty, when the person is supine (lying down) and gravity is neutral, the venous blood can exit the leg properly.
Certain conditions aggravate this inherited valve problem and make it manifest earlier in life, and/or more severely. These include: pregnancy (due to increased blood volume and hormonal changes making veins dilate more—this is why women clinically manifest vein problems more than men), being overweight or obese, working in a sedentary job, or a job in which there is much standing. The veins of the legs prefer to be worked out. Staying active during the day with frequent walking or leg movements, along with maintaining a healthy body weight are all vein-healthy. Despite this, in many people who have inherited the trait for CVI, they still manifest the pain/swelling/varicose veins at some point in their lifetime.
It is possible for CVI patients to never do damage to their tributary veins. As such, they have valve backflow (reflux) in one or more superficial trunk vein, but never have any surface varicose veins. This is a small subset of vein sufferers, but important all the same, since this subset of people can complain of chronic pain, swelling, skin problems, or restless symptoms of the legs, yet go a lifetime without vein problems being considered. In such people, a simple in-office venous ultrasound that is performed in the office can diagnose the problem, and then lead to very minor procedures to permanently eradicate the problem and associated symptoms.
Reflux
This term is used in medicine for a variety of conditions, most commonly for stomach acid reflux in to the esophagus (causing “heartburn”). In vein medicine, the term reflux is used for the backflow in to veins in the legs due to the faulty valves, much worse when gravity is at play, and progressive over time.
Ultrasound
Synonymously, ultrasound is referred to as “sonography” or “ultrasonography”. Ultrasound uses sound waves transmitted through a medium to return a visual image. In the case of vein medicine, the medium is the tissues of the leg. Formally, the term for the type of ultrasound performed in vein medicine is “venous duplex ultrasound”. To properly diagnose the presence or absence of abnormal venous flow in the leg, the patient should be in a standing position. Ultrasound has revolutionized the field of modern vein medicine, allowing the practitioner to precisely diagnose the parts of the venous system of the leg that is malfunctioning. Ultrasound is also a key part of the modern procedures, including laser, to visualize all steps needed below the skin surface.
Thrombophlebitis
This term is commonly shortened to “Phlebitis”. This refers to an active blood clot and secondary inflammation of the vein wall due to the clot. Thrombophlebitis can occur in both superficial and deep veins of the legs. Typically, thrombophlebitis of the deep veins is a much more serious condition and can be limb or life threatening. Certain medical conditions, surgery involving general anesthesia, and prolonged inactivity are the biggest risks for deep vein clots. Fortunately, most people with superficial CVI with/without varicose veins, are NOT at increased risk of deep vein clots. They are, however, more prone to thrombophlebitis of the superficial veins, due to stagnation of vein return of the legs in these superficial veins. Superficial thrombophlebitis is very painful, usually causes a hard, red, hot, very tender area on the leg. There is no quick fix to make this problem go away and episode can take weeks-months to resolve. Anti-inflammatories and moist heat can help calm the pain. Once a CVI patient experiences their first episode of thrombophlebitis, they are at increased risk of suffering repeat bouts. If the CVI is corrected with the minor surgical procedures performed routinely at Vein Specialists of Alaska, the risk of future superficial thrombophlebitis is negated.

 Perforator Veins
Perforator Veins
(a.k.a. Connector Veins)
Perforator veins (PV) are the auxillary vein drainage system in each leg that we all have that functions from the time we are born. There are about 100 PV in each leg, and they serve as another route for blood to get from the superficial veins (skin down to muscle layer) to the deep veins (all located in the muscles of the legs). If you can picture a ladder laid on its side with the top rail of ladder being a superficial vein (either branch or trunk vein), and the bottom rail of ladder being a branch or trunk deep vein, the PV is a very short vein, looking like a rung of the ladder, connecting the superficial “rail” vein to the deep “rail” vein. PV (connector veins) are valved, and if functioning properly, allow vein blood to flow one way from the superficial veins to the deep veins. For proper clearance of the venous blood of the legs, it must travel from superficial veins to deep veins, and then muscle movements and valve opening/closing allow the blood in the deep veins to exit the legs and return to the heart. Once diseased back-flowing major channels and branches of the superficial system are eliminated (usually either the GSV or SSV) by the modern techniques we employ at VSA, it is the PV system that steps up to carry the blood from that area of superficial drainage to the deep venous system. Without the PV system, modern vein procedures (or its predecessor—vein stripping) would not have been possible. Without the PV system, venous blood would have no auxiliary route to the deep vein system and then out of the leg.
Telangiectasias
The medical term for Spider Veins. Spider veins occur due to valve failure in the Reticular Veins. Typically only sections of these veins will develop faulty valves. In these areas, excessive pressure builds up inside the reticular veins, again mostly when the person is in a gravity dependent position. Spider veins form in these areas of faulty reticular veins literally like a “pop-off valve” to release the extra pressure. The bad of this pressure release is that the spider veins are unsightly from a cosmetic standpoint, and in some sufferers cause burning and stinging discomfort. The genetics for spider veins, like varicose veins, runs in families. Family lineage can have the genetics for spider veins only, varicose veins only, or both. Similar to varicose sufferers, those with spider veins tend to be worse affected if they work in professions that require prolonged sitting or standing.
Restless Leg Syndrome (RLS)
This is a common malady that is strongly related to vein disease of the legs. Click here for detailed explanation.
Lymphedema
Most of the swelling in the legs from venous disease is actually due to lymphedema—impaired drainage of the other drainage system of the legs, the lymphatic system. The vessels of the lymphatic system, compared to veins, are much smaller and rice paper thin. As such, they are very sensitive to even slight pressure changes, such as occurs with worsening Chronic Venous Insufficiency (CVI), especially in the lower legs, ankles, feet. In the majority of patients seen at Vein Specialists of Alaska, the lymphedema is due to underlying vein disease (termed secondary lymphedema); however it is possible to inherit a faulty lymphatic system in the absence of vein disease (termed primary lymphedema). The simple office ultrasound performed at Vein Specialists of Alaska can show if lumphedema is the primary or secondary type. Specialized lymphedema therapy is available by certified therapists to reduce the swelling and improve skin quality, but if CVI is involved, it will not meaningfully improve with correcting the venous problem via the minor surgical procedures performed routinely at Vein Specialists of Alaska.
If venous disease of the legs is advanced by the time of intervention (i.e. “C” class C4, C5, or C6, see medical classifications), a small but significant percentage of these patients will have refractory lymphedema that is either constant or recurring in an ebb/flow pattern. For such patients, lymphedema therapy on a PRN (as needed) basis, chronic compression therapy, and/or an automatic lymphedema therapy machine (such as the Flexitouch®) can be very useful.